
Osteoarthritis treatment: Houston, we have a problem
Osteoarthritis is the main cause of pain and physical disability in the elderly, increasing greatly with age. Hygienic and dietetic measures are fundamental, especially the control of overweight and obesity, which on many occasions are complicated to carry out in patients with permanent disability, the main treatment being surgery.
The different clinical practice guidelines that assess osteoarthritis pain in the elderly emphasize the use of paracetamol, with a grade of recommendation A, due to the multiple digestive and cardiovascular alerts of anti-inflammatory drugs (NSAIDs and coxib). The continuous or intermittent use of NSAIDs is very frequent in the geriatric population, often polymedicated, with the risks of interactions and renal alterations that it entails.
In an article published in the Lancet in March of this year*, a Swiss research group carried out a meta-analysis evaluating therapeutic interventions (7 groups of NSAIDs, paracetamol or placebo) in the management of pain and dependency produced by osteoarthritis, including 74 clinical trials from 1980 to 2015, with 58,556 patients with an average age of 58 to 71 years, 49 to 90% women and with a follow-up of around 12 weeks. The most studied drugs in the clinical trials are celecoxib at 200 mg/day and naproxen at 1000 mg/day.
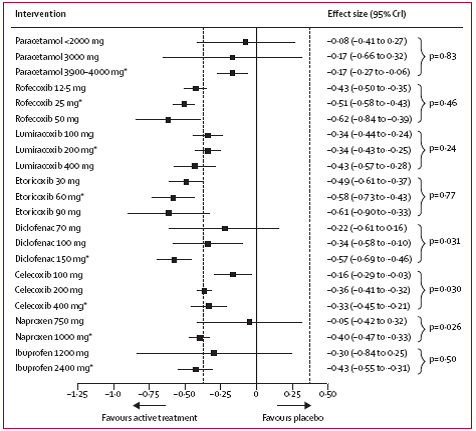
With regard to pain control, diclofenac at a dose of 150 mg/day and etoricoxib 60 mg/day are the most effective (Table 1); while in functional recovery diclofenac 150 mg/day and rofecoxib 25 mg/day stand out. (Table 2)
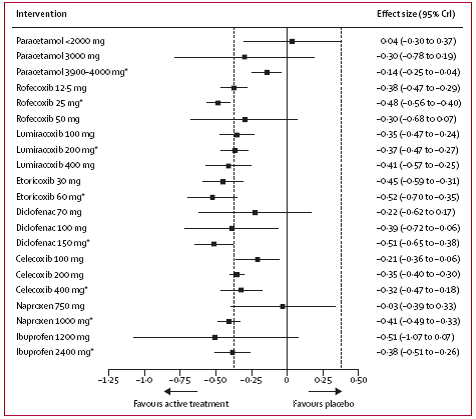
Both paracetamol at different doses (<2000 mg, 3000 mg, 3000-4000 mg), and low-dose NSAID guidelines such as diclofenac 75 mg, naproxen 750 mg or ibuprofen 1200 mg/day are not superior to placebo in pain or functional dependence.
If we consider, as reflected in a previous entry, that paracetamol at a dose of 3 g/day maintained over time, increases the risk of hepatotoxicity four times without knowing well the clinical value that it really represents, but what seems increasingly likely is the low effectiveness of such a measure.
Pain and disability are priority objectives in the treatment of geriatric patients in order to guarantee the highest possible quality of life, balancing it with the safety of the measures in place. The main thing is to carry out a complete and dynamic assessment of the pain, periodically evaluating the effectiveness of the interventions, as well as implementing hygienic and functional measures. In the event of pain or permanent limitation secondary to gonarthrosis or coxarthrosis, it is essential to coordinate with the traumatology services to evaluate the ideal moment for the surgical intervention in accordance with the care objectives, as always. Without forgetting that in pain there is a sensory and emotional component that modulates the pain, as well as the beliefs or expectations created by the different treatments, which makes it difficult to withdraw medication given the psychological dependence or uncertainty that its absence generates.
*Effectiveness of non-steroidal anti-inflammatory drugs for the treatment of pain in knee and hip osteoarthritis: a network meta-analysis. The lancet, published online March 17; doi 10.1016/50140-6736(16)30002-2.

Add new comment